Electronic health records as a blockchain use case
How ledger designs interact with record exchange, version control, and the audit obligations that already govern clinical records.
What this use case covers
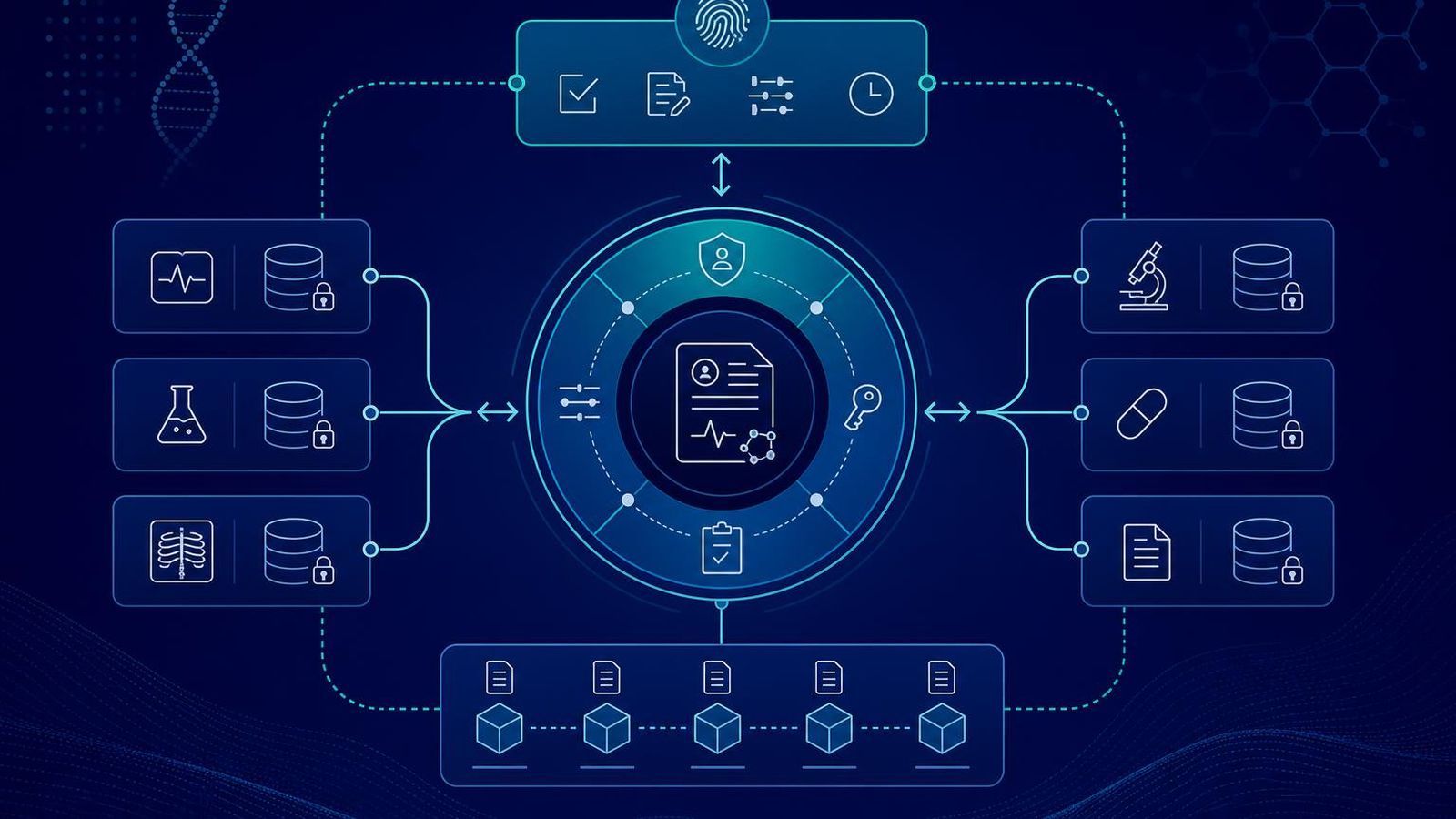
Electronic health record (EHR) projects in the directory are those whose primary purpose is to support the storage, exchange, versioning, or controlled access of clinical records using ledger-backed components. The category does not require the record itself to be on chain. In most credible designs the record stays in its existing storage system and the ledger carries commitments, consent receipts, access logs, and version pointers.
What it does not cover
Pure consent dashboards without an EHR connection are categorised under consent management. Patient identity work is categorised under patient identity. Pure provenance work for research datasets is categorised under research data provenance. The boundaries are not always crisp, and projects that operate across categories are listed in each.
Recurring design patterns
The pattern that recurs in credible EHR projects is off-chain storage with on-chain commitments. The record stays under the access controls that already govern it. The ledger records the existence of a specific version, the consent state attached to it, and the access events that touch it. Amendments are handled as supersedence with explicit version links. Deletion is handled at the storage layer with a tamper-evident gap in the audit log.
Implementation realities
Integration with existing exchange standards is non-optional. A project that does not integrate is not exchanging records. Vocabulary mapping, identifier resolution, and message format support all have to be present. The chain choice is downstream of the integration strategy. Projects that pick a chain first and figure out integration later tend to redesign the chain choice once the integration constraints are understood.
What the directory looks for
Projects in this category are categorised on the maturity of their deployment, the clarity of their integration story, the seriousness of their privacy posture, and the realism of their patient-control claims. Inclusion is not endorsement. Confidence labels reflect the evidence available, and the methodology page describes how the labels are assigned.